INTRODUCTION
Bell palsy is the most-common type of peripheral facial palsy in children; however, peripheral facial palsy could also signal the presence of a severe underlying disease.[1] Facial nerve palsy (FNP) term is used when the paralysis is thought to be the result of a particular disease process. parotidectomy was first introduced into the world literature by Berard in 1823 who removed a parotid tumor of 8 years’ duration. It has been associated with various causes such as strokes, acoustic nerve tumors, diabetes mellitus, multiple sclerosis, Lyme disease, pregnancy, trauma, and viral infections including Herpes-Zoster. Dental causes have also been reported with facial paralysis in few cases,[2-4] such as orofacial granulomatosis, maxillo-facial surgical procedures (both intra- and extra-oral) and even fracture of the mandibular condylar neck.[5-8] It has also been associated with human immunodeficiency virus infected patients.[9,10] This case reports highlights the right facial palsy in 55-year-old female patient secondary to radical mastoidectomy with partial parotidectomy. Postoperative complications following parotidectomy are well-documented and include complications such as facial nerve paresis or paralysis, salivary fistula, Frey’s syndrome, infection, and recurrence of the tumor. Parotid gland surgery complications can affect the quality-of-life and are potentially disfiguring.[11]
CASE REPORT
The case we present here is about a 55-year-old female patient who was reported to the Department of Oral Medicine and Radiology with the chief complaint of decayed tooth in the left lower back region of the mouth that was not associated with pain or any other symptoms. The past medical history revealed that she had undergone right radical mastoidectomy with partial parotidectomy for adenocystic carcinoma of the right middle ear, followed by full course of radiotherapy 4 years back. The family history, past dental history and personal history was non-contributory. On general physical examination, she was co-operative, moderately built, and nourished had a normal gait.
Extra-oral examination showed gross facial asymmetry with deviation of the face to the left during movements and at rest the patient has an expressionless face [Figure 1] (informed consent was obtained from the patient for the photographs). She also showed loss of voluntary control over eyelids with intermittent epiphora and inability to blow out right cheek. Evaluation of the muscles supplied by five branches of the facial nerve was performed. On examination of the frontalis muscle supplied by the temporal branch, the patient demonstrated inability to raise eyebrows and mild loss of horizontal folds on the right side of the forehead [Figure 2]. Examination of the orbicularis oculi muscle supplied by the zygomatic branch revealed inability to close eyelids tightly [Figure 3]. Examination of the buccinators/orbicularis oris muscle supplied by the buccal branch revealed inability to blow air. Examination of the buccinators/orbicularis or is muscle supplied by the mandibular branch revealed inability to avert her lips on the left side [Figure 4]. Examination of the platysma muscle supplied by the cervical branch of the facial nerve revealed inability to clench his teeth and grin on the left side. Examination of the other cranial nerves was normal. On intra-oral examination, salivary flow was normal and no altered taste sensation. Hard tissue examination showed decayed tooth in the left lower second molar and right lower canine and first premolar teeth. Mobility of the teeth was noticed in the right lower lateral incisor and canine with plaque and calculus deposits. We arrived at the diagnosis of facial palsy on the right side secondary to partial parotidectomy. The other diagnosis was chronic generalized periodontitis, dental caries in relation to the left lower second molar, right lower canine and first premolar teeth. Treatment plan of the patient included extraction of the mobile tooth followed by oral prophylaxis and restoration of a decayed tooth. The patient was advised to wear sunglasses during daylight to prevent corneal drying and advised periodic follow-up for every 6 months.
Figure 1
Expressionless face

Figure 2
Loss of wrinkling of the forehead on right side

Figure 3
Inability to close eyelids on the right side

Figure 4
Revealed inability to avert her lips on the right side

DISCUSSION
The facial nerve leaves the brainstem to run in the internal acoustic meatus with the eighth cranial nerve. It gives rise to various branches as it runs in the facial canal before it leaves the skull via the stylomastoid foramen. In addition to providing the motor innervation to the facial muscles, branches supply secretomotor fibers to the lacrimal gland and the submandibular ganglion, sensory fibers to the anterior two-thirds of the tongue via the chorda tympani and motor fibers to the stapedius muscle in the middle ear. The site of the seventh cranial nerve lesion can be predicted by assessing which of the branches are involved. It is also possible to determine whether the lesion is of the upper or lower motor type, as in the latter case the forehead muscles are spared because of crossover innervations at a higher level.[12]
Muscles of facial expression are innervated by the facial nerve. Two types of paralysis are noticed affecting the motor function of the facial nerve, which can be classified as a central type or a peripheral type.[13]
-
In the central type, corticobulbar fibers are involved, which convey impulses from the cerebral cortex to the cells of the motor nucleus of the facial nerve. A central lesion is interrupting the corticobulbar pathways results in paralysis only of the lower facial muscles on the opposite side of the lesion. This is explained by the fact that the corticobulbar fibers to the forehead and the upper half of the face are distributed bilaterally; however, the fibers to the lower half of the face are predominantly crossed.
-
In peripheral type, lesion of the facial nerve occurs at the level of the pons or anywhere along the distal course of the nerve. This lesion produces total facial paralysis on the same side as the lesion.
-
A peripheral lesion produces a more severe type of facial paralysis compared to the central lesion, but central lesion’s origin may represent a serious problem in the brain. To differentiate central from a peripheral lesion a simple neurological test is done in which the patient is asked to wrinkle the forehead; if the patient can wrinkle the entire forehead, the lesion is centrally located. If the patient can wrinkle only half the forehead, the lesion is peripherally located.[14] In the present case, the lesion was peripherally affected as wrinkling of the forehead was noted only on the half side of the unaffected side.
Loss of facial expression is noticed in FNP and is most commonly caused by a benign self-limiting inflammatory condition known as Bell’s palsy. The various other causes of facial palsy include microcirculatory failure of the vasonervorum, viral infection, ischemic neuropathy, autoimmune reactions, surgical procedure such as local anesthesia, tooth extraction, infections, osteotomies, preprosthethic procedures, excision of tumors or cysts, surgery of temporomandibular joint and surgical treatment of facial fractures and cleft lip/palate.[2-10,13] In the case presented, the facial paralysis was due to surgery for adenocystic carcinoma of the right middle ear with partial parotidectomy.
The clinical picture of all patients with peripheral facial palsy is identical, no matter of etiology, so they are often wrongly classified and treated as Bell’s palsy. The severity of signs and symptoms vary considerably. The palsy is characterized by an abrupt loss of muscular control on one side of the face, imparting a rigid mask-like appearance and resulting in an inability to smile, to close the eye, to wink, or to raise an eyebrow. The corner of the mouth usually droops, causing saliva to drool onto the skin. Speech becomes slurred, and taste may be abnormal. Because the eyelid cannot be close, conjunctival dryness or ulceration may occur.[14] Similar features were noticed in our case. The most popular method for assessing the severity or paralysis is the facial nerve grading system according to House and Brackmann [Table 1].[15]
Table 1
The House-Brackmann grading system
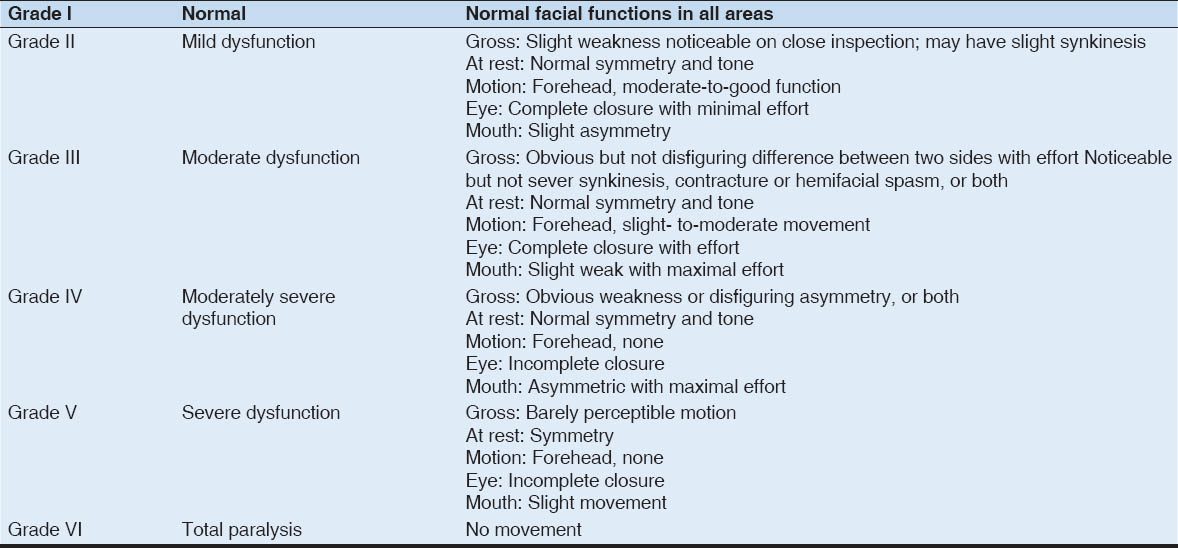
In the present case, we graded it as moderately dysfunction.
No universal preferred treatment exists for Bell’s palsy.[14] There is evidence to support prednisolone therapy in the treatment of Bell’s palsy, and it has been reported that delay in initiation of steroid treatment can adversely affect the outcome. Combination treatment with acyclovir and corticosteroids may improve the outcome in idiopathic facial nerve paralysis. Physiotherapy, in the form of transcutaneous peripheral nerve stimulation, has an important role. If the FNP results in weakness of the eyelids the eye must be protected. In the short term, patches are useful, as are chloramphenicol eye drops or ointment, and tarsorrhaphy is indicated when recovery is prolonged.[12] In the present case, facial palsy was secondary to partial parotidectomy, no treatment option was available. The patient was advised to wear sunglasses during daylight to prevent corneal drying and advised ophthalmic follow-up. The avoidance of washing out of the wound with powerful antiseptics combined with the limitations in the indications for total parotidectomies provides an obvious explanation for the reduced incidence of major functional paralysis.[16]
Fareed et al. 2014[17] researched and adopted certain precautions to lower the incidence of temporary facial nerve paresis. One of these precautions is a vertical retraction to reduce the risk of traction injury. Once the nerve trunk was identified we did not use diathermy at all; hemostasis was performed with surgical ligatures (5/0 polygalactin).
CONCLUSION
Unilateral facial palsy is usually idiopathic or related to viral illness. Very few cases of facial palsy are reported as a post-operative complication of surgery any pathology involving the parotid gland or surrounding structures. This paper attempts to highlight a case of unilateral facial palsy in a 55-year-old female secondary to partial parotidectomy.