INTRODUCTION
Oral myiasis is a word derived from Greek word “myia” which means invasion of vital tissue by fly larvae (maggots) as is means disease in humans or other mammals.[1,2] Initially, it was described by Laurence in 1909[3] and term coined by F W Hope, after this Zumpt[4,5] defined it as parasitic infestation of house fly (in adult form) in live human and vertebrate animals by diptera larvae and this larvae or maggots feed for a certain period of time on host’s dead or living tissue, liquid body substance, and ingested food. Almost 86 different species of flies have been reported to cause human myiasis. A condition similar to myiasis was considered by the Hindu mythology as “God’s” punishment to sinners. On removal of the larvae, the tissues seem to recover with no subsequent complications and with no need for further treatment. Here, we describe two cases of oral myiasis within the gingiva (Intra-oral) of a small child and extra-oral in an adult caused due to bad oral hygiene maintenance, low socioeconomic status of both patients, Untreated traumatic injury to face further which leads to infection to both the patients and maggots may have been developed due to bad oral hygiene, ingestion of infested flesh etc. In both Patients after applying of turpentine for 15-20 minutes maggots were removed with the help of tweezers and haemostat. For Case 2 further management was planned for surgical debridement of dead necrotic tissue and irrigation with saline and betadine but unfortunately patients didn’t turn up on review appointments. In the case of maggot infestation, larvae may infect dead, prematurely dying, or sometimes even living tissue. The infestation of tissue by larvae can take place in various parts of the human body such as stomach, skin, ears, intestinal tract, and eyes[6,7]. They generally invade open or surface wounds, unhealed wound (untreated traumatic wound), or skin with cuts or are broken in some manner. The egg hatches within 24 h and the larvae [Figure 1] burrow inside the host’s tissue with head downward into the wound in a screw-like fashion. Hence the name “screw worm.”
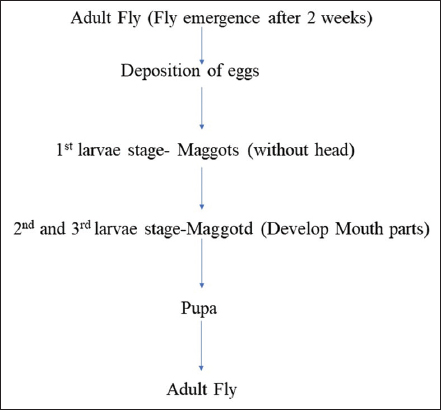
Figure 1: Patients gender distribution
CASE REPORT
Case Report 1
A 2-year-old infant visited to the department of dental surgery with the complaints of swelling in the upper lip and gingiva and in upper alveolus with pain for 3–5 days. Presence of worms [Figures 2 and 3] and swelling in upper maxillary gingiva was reported in his mouth by the parents. He presented with persistent mouth opening and poor oral hygiene. Intraoral examination revealed a 0.5 cm by 1.0 cm perforation of the anterior palate, about 2 mm from the gingival margin of the upper right central incisor. The cavity was filled with numerous maggots.
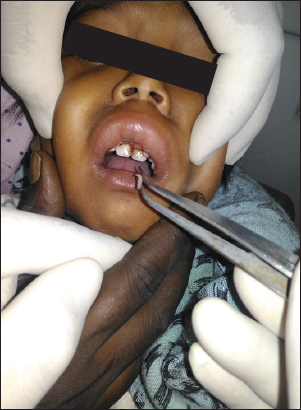
Figure 2: Etiology of mandibular fracture

Figure 3: Status of occlusion in both the groups
The first attempt was to flush the cavity with normal saline which proved ineffective. A cotton bud impregnated with turpentine was then placed at the opening of the cavity for 10–15 min. Dozens of maggots “rushed” [Figure 4] out from the cavity. This procedure was performed out twice daily.

Figure 4: Comparison of pain in both groups
By the 3rd day, the oral cavity was free from maggots after 1-week follow-up [Figure 5].

Figure 5: Comparison of swelling in both groups
Case Report 2
A 35-year-old male visited to the department of dental surgery with a complaint of swelling and coming out of worms from lower jaw for 2–3 days. This male patient presented in dept of dental surgery with extra-oral huge swelling and sensation of crawling of worms on lower mandibular region for 4-5 months. He gives the history of trauma on face 5 months back which was left untreated due to lack of money. He was with normal mouth opening but poor oral hygiene with unpleasant odour. Routine blood investigation was in normal limits and radiograph OPG revelled no signs of mandibular fracture. Based on maggot’s findings and history provisional diagnosis oral myiasis was made.
In both cases the patient and relatives were informed and informed consent was taken. He is a rickshaw driver and lives with his elderly mother, was unmarried and neglected his traumatic open wound due to lack of money and his poor condition. The same cleansing method was used to treat the patient, but even after numerous motivation patient failed to attend the dept for review appointment [Figures 6-8].

Figure 6: Anatomic distribution of mandibular fracture

Figure 7: Showing Applying Turpentine at the place of maggots

Figure 8: Showing Removed larvae
As in the first case, the cavity was filled with maggots. The same method of cleansing was performed. It took 2 days to get the cavity cleaned and free from the maggots. He was then discharged. He too failed to attend the review appointment.
For both cases, broad spectrum amoxycillin 250 mg (for child) and 625 mg (adult dose) three times daily was prescribed as there were signs of infection. Post application of turpentine oil maintenance of oral hygiene instructions and reinforcement (to the both parents and guardians) was carried out extensively. The parents and guardians were given extensive hygiene instruction and reinforcements.
DISCUSSION
The myiasis larvae can develop in two clinical cases: Obligate parasites, which thrive on living tissues, and facultative parasites, which attack necrotic tissues and wounds. The larvae generally found in necrotic lesions (cavitary myiasis) are from the genera: Sarcophaga, Lucilia, Calliphora, and Musca.
The most common form of myiasis in men takes place in the skin, where the species Dermatobia hominis is mostly observed. The severity of the condition depends on the location and on the degree of tissue destruction.[9-11] Psychoda albipennis is an insect species that causes urogenital myiasis in humans. Adult forms of this species belong to the Psychodidae subfamily and live, especially, in humid toilets and domestic bathrooms.[10] Flies are attracted to malodor and suppurative lesions where they lay their eggs and develop into larvae. The pathogenicity results from inflammation and toxins secreted by the larvae. The larvae are photophobic, penetrating deep into the tissues with the help of sharp mouth hooks. Genitourinary infestation usually presents as pain and pruritus at the site.[8-11] Transmission occurs through the accidental deposit of eggs on oral or other openings or by swallowing eggs or larvae that are present on food.[9]
Primary myiasis (active invasion) is caused by W. magnifica also known as screwworm whose biophagous larvae (feed on living tissues) and also called as obligatory myiasis. Secondary myiasis (colonization of wound) is caused by the necrobiophagous larvae (feed on dead tissues) and also called as facultative myiasis.[8,9] The most common anatomical sites for myiasis are the nose, eyes, skin wounds, sinuses, ears, lungs, gut, gallbladder, vagina, nasal cavities, and rarely, the mouth.[10] Whereas, cutaneous myiasis involves invasion of the skin through the wounds. However, specific types of flies can even penetrate healthy skin and produce myiasis.[11]
The common predisposing factors are incompetent lips, poor oral hygiene, severe halitosis, anterior open bite, mouth breathing during sleep, facial trauma, extraction wounds, ulcerative lesions, and carcinoma.[12,13] Most of the patients are senile,[14] alcoholics, mentally handicapped,[15] cerebral palsied,[12,14-15] and also those living in poor conditions, with no age limitation.[8] Droma et al.[7] reported that incidence of myiasis is more in anterior maxillary region and men are more affected than women. Traumatic wounds in orofacial region, when neglected by patients themselves as well as caretakers, can lead to the development of myiasis.[13,16]
If a screwworm or fly deposits its eggs on mucous membranes, the larvae may enter any orifice including the nostrils, sinuses, mouth, orbits of the eye, ears or genitalia and can cause infections of the skin, gut, bladder, nasal cavities, aural cavities, eyes and occasionally the oral cavity.
Treatment of myiasis comprises of various systemic and local measures including motivation of patients that it is curable within certain time.
Local measures to be followed in Myiasis are-
-
Broad Spectrum Antibiotics
-
Application of turpentine Drug for e.g mineral oil, ether, chloroform, Saline, creosote ethyl chloride, mercuric chloride, thiobendazole or systemic butazolidine. Turpentine is toxic chemical which can cause tissue necrosis (ulceration, hyperkeratosis, epithelial hyperplasia) however the cause is reversible.
Systemic Measures to be followed are as-
-
Debridement’s of Maggots till all maggots came out
-
Maintenance of oral hygiene
-
Regular Follow up
CONCLUSION
The occurrence of oral myiasis in the oral mucosa is rare, especially when associated with poor oral hygiene. This condition mainly affects patients with a very low socioeconomic status, characterized by poor hygienic habits. Poorer patients with less education tend to delay longer in seeking medical care, and therefore, the diagnosis of the disease is frequently performed in advanced stages. Treatment is usually repeated at intervals until the wound has healed. Removal of necrotic tissue may be necessary, and antibiotics may be given when secondary bacterial contamination is present