INTRODUCTION
The essences of cleanliness were captured by the Dravidians, who in 5000 B.C gave due emphasis to safe and effective sewerage systems, to get rid of all solid and liquid waste generated by the population. They were indeed the pioneers as far as scientific waste management is considered.[1]
World Health Organization (WHO) defines health-care waste as total waste generated by Hospitals, health-care establishments, and research facilities in the diagnosis, treatment, or Immunization of human beings or animals, and other associated research and services.[2]
According to notification, 1998 of the Government of India it has been specified that Hospital Waste Management is part of hospital hygiene and maintenance activities. This involves management of arrange of activities, which are mainly engineering functions, such as collection, transportation, operation/treatment of processing systems, and disposal of waste. However, initial segregation and storage activities are the direct responsibility of nursing personnel who are engaged in the hospital.[3]
More than 3–4th of the health-care wastes are nonhazardous while the remaining proportion is potentially hazardous. According to the WHO, 20% of total waste generated by health-care activities are hazardous.[4]
Dental offices generate a number of hazardous wastes that can be detrimental to the environment if not properly managed. This includes sharps, used disposable items, infectious wastes (blood-soaked cotton, gauze, etc.), mercury-containing waste (mercury, amalgam scrap), lead-containing waste (lead foil packets and lead aprons), and chemical waste (such as spent film developers, fixers, and disinfectants).[5]
The success of biomedical waste management program depends on the knowledge and practice of the Health Care Worker (HCW).[5]
With this background, the purpose of this study was to evaluate the practical calibration and awareness of dentist and auxiliaries in disposal of hazardous biomedical waste generated during dental treatment into color-coded disposing bags at dental hospital so that depending on their attitude they can be motivated to attend training and CDE programs concerning waste management so that they will be efficient to properly segregate, disinfect and dispose hospital waste in an eco-friendly way.
Aim
The aim of the study was to assess:
-
Awareness’ toward waste management policy and practices.
-
Approach toward waste management policy and practices.
-
Performance in waste management policy and practices among the private dental practitioners in the city of Vellore, India.
MATERIALS AND METHODS
Study Design, Area, Duration, and Populations
The study was a cross-sectional questionnaire-based survey which was conducted to identify the exact management problems related to the segregation, collection, transportation, and disposal of hospital waste.
The study design among general dental practitioners and dental specialists was practicing in and around Vellore, Tamil Nadu State excluding house surgeons, non-practicing dentists or dentists with the administrative job only. Data were collected during the months of October 2017–December 2017.
Inclusion Criteria and Exclusion Criteria
-
Inclusion criteria: Dentists enrolled as a private dental practitioner, willing to participate and registered in Tamil Nadu State Dental Directory were included in the study.
-
Exclusion criteria: Dental Practitioner who were not willing to participate, dental students under internship and private dental practitioners who were in pilot study were excluded from the study.
Sample size and techniques
A total coverage of dentists working in private clinics in Vellore and surrounding locality were involved. Lists of all private dental clinics were obtained from the directory. The total number was 150 registered and practicing dentists.
Survey Tool
The study was conducted using pre-designed, pre-tested, semi-structured, interview schedule, self-administered, and open-ended (27) close-ended (24) questionnaire with a letter explaining, the purpose of the study was distributed by the researcher. It was handed to the participants during evening clinics hours. The questionnaire originally developed by Umar and Yaro,[6] with some modifications.
In the present investigation, first of all, an extensive pilot study was carried out at 15 dental clinics of the above-mentioned strata which were selected by random sampling technique. The pilot study provided the basic data on which the biomedical waste management system was premeditated, designed, and operated in each facility.
Participants were requested to participate voluntary after explanation of the purposes of the study. Informed written consent for their participation was obtained, and confidentiality of responses was assured.
The questionnaire was formulated into four parts:
Questionnaire: It consisted of 51 questionnaires with 2–5 responses. They were further categorized into five sections.
Part One
It consisted 5 questions of demographic division and qualification data. Dentists were asked about, age, Academic Qualifications, and years of working in Dental Clinic or Hospital.
Part Two
It consisted of 7 questions based on the assessment of knowledge on Biomedical Waste Management Policies and practice.
Part Three
Response consisted of 12 questions based questions on Biomedical Waste management.
Part Four
Response consisted of 27 questions based on Practices Biomedical Waste Management (Attitude assessment).
Part Five
Response consisted of one question based on Preventive measures taken by the health-care professionals while handling BioMedical Waste.
Participants answered the questionnaire and returned them to the researcher at the same day or the day after. It took 10–15 min to answer all questions.
Data Analysis
Data were analyzed by SPSS Version 21 (SPSS Inc., Chicago, USA). Results were presented in form of tables and figures. Comparison between variables assessed using Chi-square and Pearson correlation tests with the level of statistical significance set at P = 0.05.
RESULTS
The Profiles of Respondents - Table 1
Table 1: Social -demographic variables of respondents
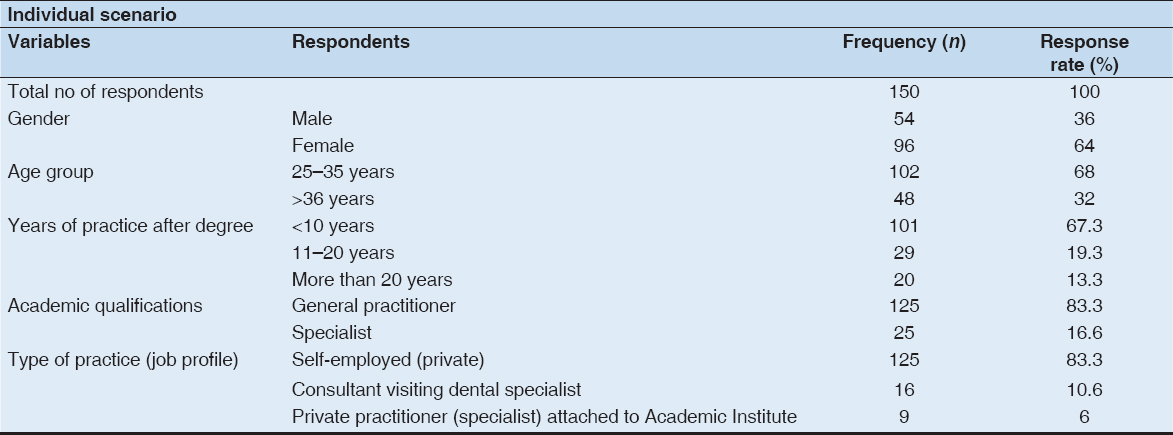
Descriptive statistic of the results showed that response rate was 100% (150), the percentage of males was 36% (n = 54) and rest 64 % (n = 96) females.
The age group of participants ranged between 25 years and above. Majority of the participants in the present study belonged to age group 25–35 years 68% (n = 102).
Majority of the participants 67% (n = 101) had <10 years practice experience and 83.3% (n = 125) were general dental practitioners.
Biomedical Waste Management Policies - Table 2
Table 2: Biomedical waste management policies
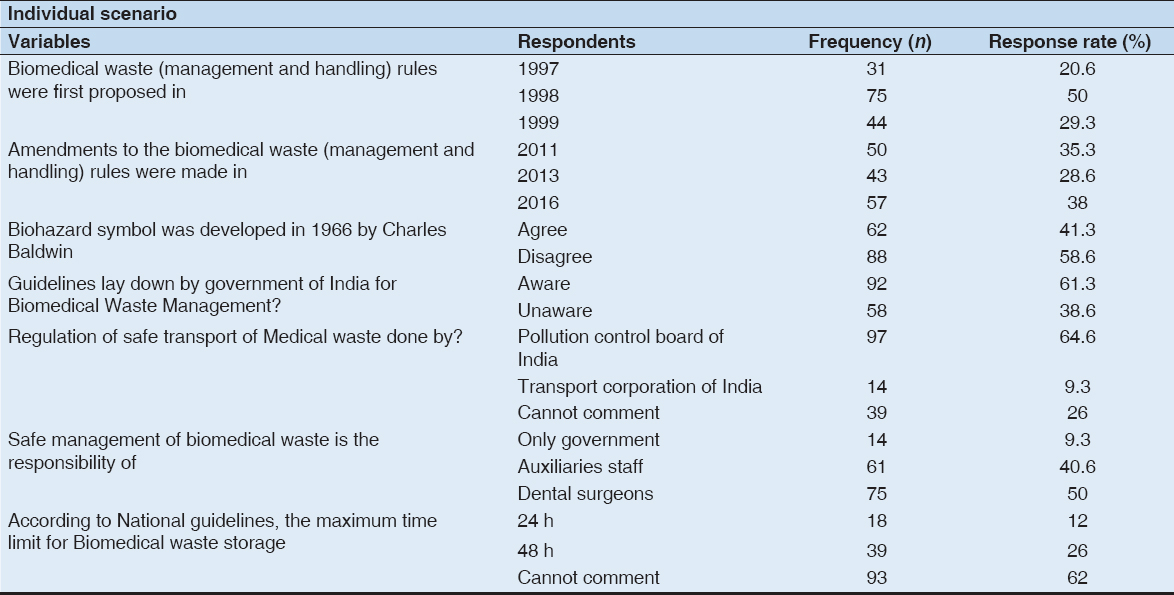
Although majority 61% (n = 92) dentist had heard about guidelines lay down by the Government of India for Biomedical Waste Management, only 50% (n = 75) were aware of Biomedical Waste (Management and Handling) Rules, 1998 and its Amendments rules were made in 1998.
Response to Knowledge-Based Questions on Biomedical Waste Management -Table 3
Table 3: Response to knowledge based questions on biomedical waste management
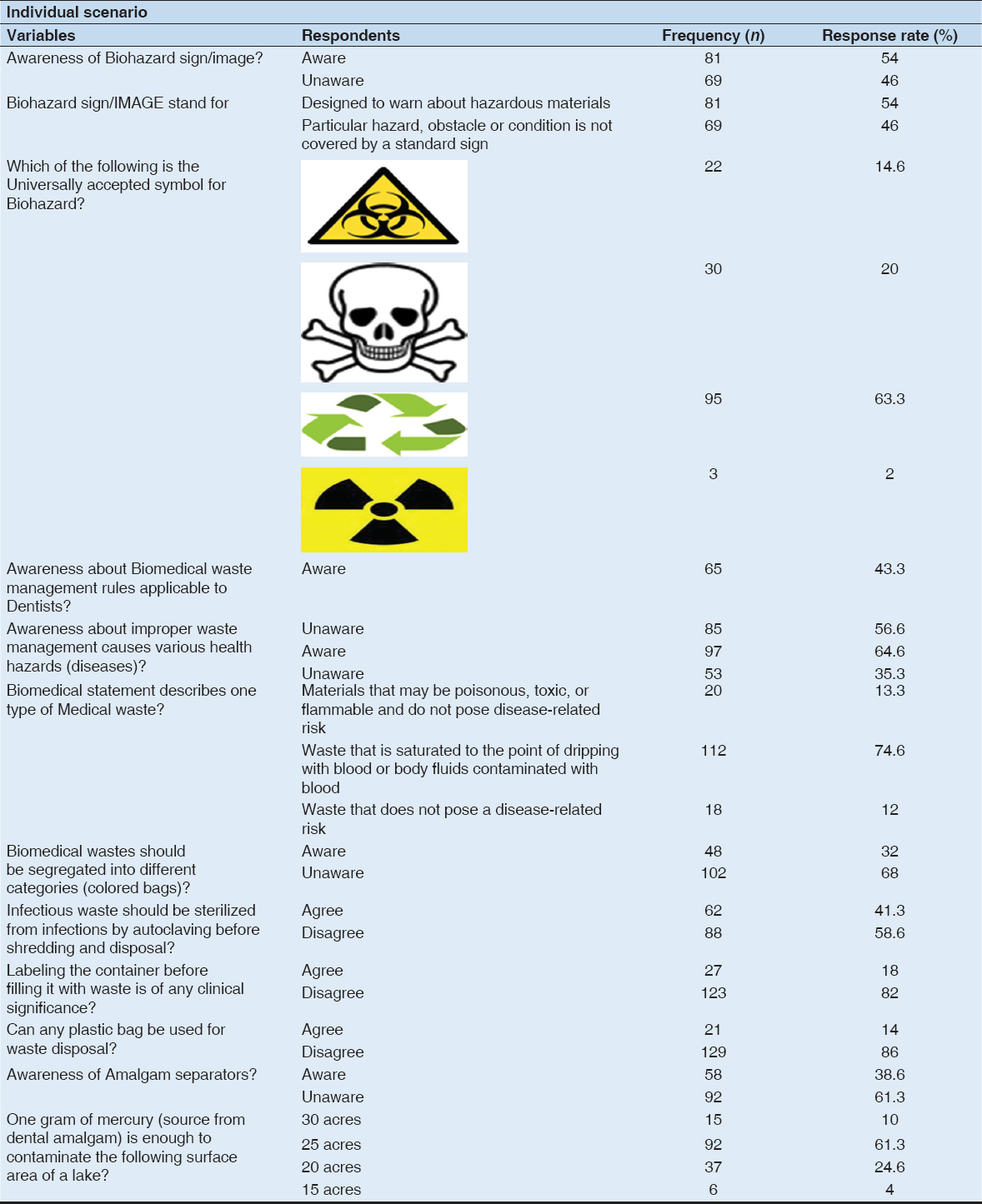
About 64.6% (n = 97) of the respondents considered all health-care wastes hazardous.
Only 54% (n = 81) were aware of Indian Medical Association Goes Eco-friendly (IMAGE), and of them, only 25% (n = 38) knew the correct expansion of the abbreviation of IMAGE. Around 54% (n = 81) of the respondents correctly recognized the symbol of biohazard.
41% (n = 62) were reported for disinfection of BMW before disposal among them.
Responses to Practice-Based Questions on Biomedical Waste Management - Table 4
Table 4: Response based on practices biomedical waste management
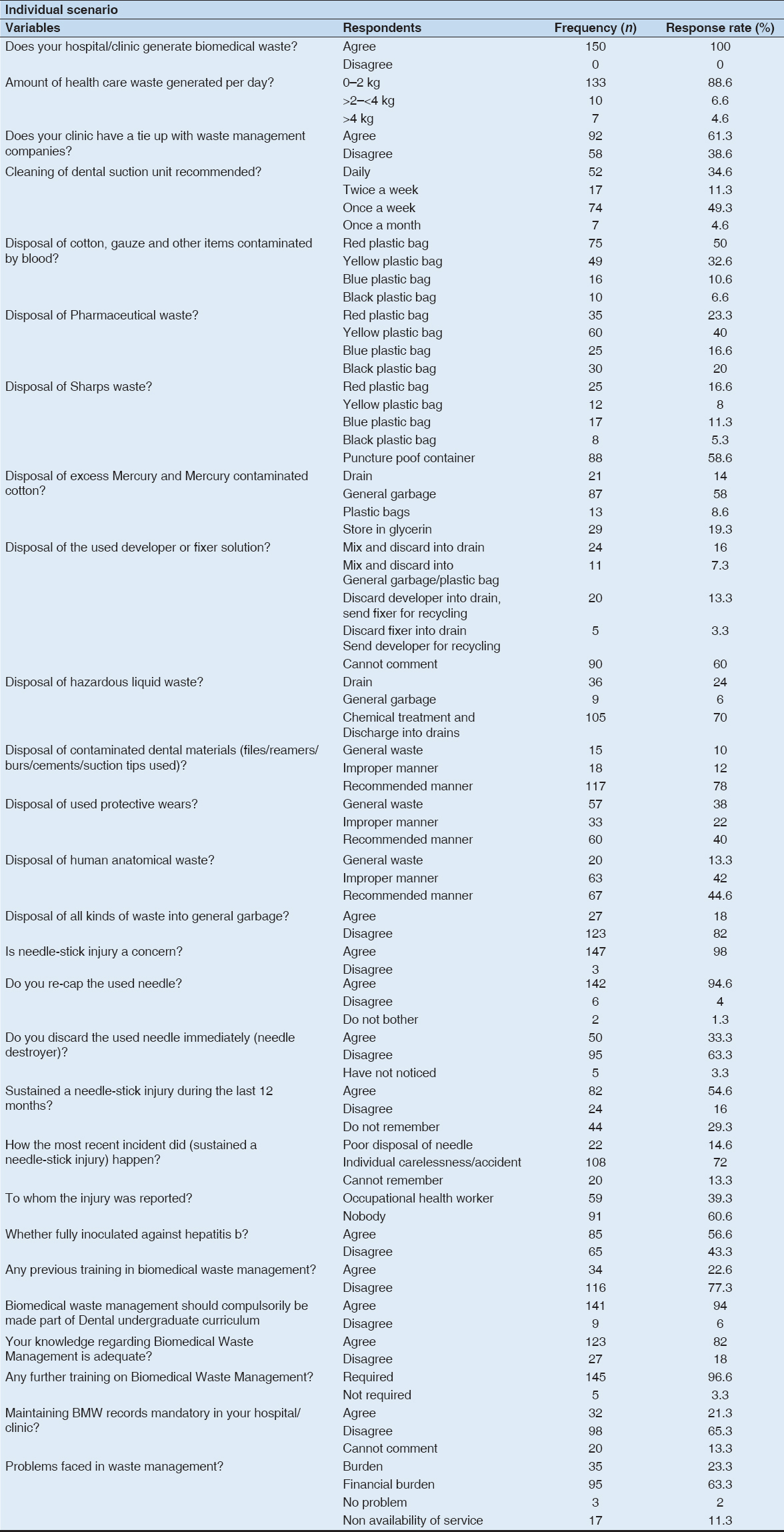
The knowledge about waste management guidelines has a significant influence on disposal of dental material 78% (n = 117), on disposal of protective wears 40% (n = 60), and human anatomical wastes 44% (n = 67).
It was interesting to note that most injuries 72% (n = 108) occurred during giving an injection, which is the most important step of the procedure. These were concerned by injuries needle 98% (n = 147).
With regard to prevention by Hepatitis B vaccine, 56.6% (n = 85) of the respondents knew about it and were inoculated.
The most common problem encountered in managing the dental health-care waste was extra expenses, 63.3% (n = 95) of the respondents believed that safe management efforts will increase the financial burden.
Preventive Measures Taken by the Health-care Professionals While Handling Biomedical Waste - Table 5
Table 5: Preventive measures taken by the health care professionals while handling Bio Medical Waste
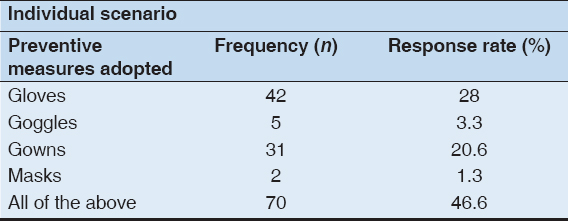
Use of personal protective measures while handling biomedical waste was adequate among doctors 46.6% (n = 70).
DISCUSSION
The survey presents a grim picture. The study revealed several lacunae in the knowledge, attitudes, and practices among the health professionals. Health professionals have an ethical responsibility toward the environment and themselves. Due to the nature of their profession, they must not forget that they are at risk for treating patients who may have infectious diseases. Dentists, dental assistants, and patients may be exposed to pathogenic microorganisms localized in the oral cavity and respiratory tract, including Cytomegalovirus, HBV, HCV, Herpes simplex virus type 1 and 2, HIV, Mycobacterium tuberculosis, Staphylococci, Streptococci, and other viruses and bacteria.[7]
These microorganisms can be transmitted to dental health-care professionals by direct contact with a patient’s saliva, blood, skin, or oral secretions, or by indirect contact through injuries caused by contaminated sharp instruments, or by droplet infection from aerosols or spatter.[8]
Self-reported awareness about the biomedical waste management system among dentists in the present study (100%) was good.
Although the self-reported awareness was high, as much as 38.6% dentists were not registered at the local governing body. Those who had not registered were disposing of waste more commonly in dustbins.
Today, hospitals/clinics use a wide variety of drugs including antibiotics, cytotoxics, corrosive chemicals, and radioactive substances, which ultimately become part of hospital waste.
The introduction of disposables in hospitals has brought in its wake many ills such as inappropriate recycling, unauthorized and illegal re-use, and an increase in the quantity of waste.[9]
The biomedical waste generated by hospitals and clinics can be broadly categorized as general waste, infectious waste, and non-infectious but hazardous waste. About 75–85% of waste generated in hospitals is a non-risk or general waste, which constitutes paper, cardboard boxes, plastic packaging, and kitchen waste. Infectious waste, which includes human anatomical wastes, infectious disposable plastic items, and sharps accounts for only remaining 10–15% of total volume of waste generated in a hospital. Non-infectious but hazardous waste includes chemical waste, genotoxic waste, and radioactive waste which comprises about 5–10% of total volume of generated hospital waste.[10]
Sushma et al. study showed that a substantial percentage of practitioners (47.9%) dispose dental waste without segregation and prior disinfection which exposes garbage collectors to a high risk of getting infected from health-care waste which was in accordance with the (64.4%) present study.[11,12]
The Ministry of Environment and Forests, Government of India has notified the new draft Biomedical Waste (Management and Handling) Rules, 2011 under the Environment Protection Act, 1986 to replace the earlier Biomedical Waste (Management and Handling) Rules, 1998 and amendments thereof.[13] These rules were aware by the HCW of the present study (61.3%).
Regarding the maximum time limit for storage of biomedical waste according to national guidelines, they were not aware of the time limit (62%) and were aware of the fact that it was 48 h which was similar to study by Sood et al.[14]
IMAGE is the scheme of IMA, Kerala, for the scientific disposal of biomedical waste. IMAGE provides comprehensive service by providing training to hospital staff for segregation of biomedical waste in color-coded bags, collection of it from hospitals, transportation in specially designed covered vehicles, scientific treatment, and final disposal in the common facility.[15] The participants were aware of the IMAGES in the present study.
In a study by Kishore et al. conducted a study in a teaching hospital in New Delhi some 12 years ago, only 35.9% of respondents were aware of this.[16] However, the guidelines laid down by Government of India for biomedical waste management were concerned; it was reassuring to note that only 43.3% of the dentists were aware of the legislation applicable to hospital waste management.
More than 68% of the HCW had no knowledge about the type of waste to be collected in black, red, or yellow colored bags related to the present study. These findings were similar to the studies done by Patil et al.[17] (72.5%).
Only 14% of the respondents including the dental students opined that any plastic bag can be used for waste segregation. The observation is in contrast with the results of studies done by Charania et al.[18] and Sudhir et al.[19] where the corresponding values were 28% and 27%, respectively.
Knowledge about color coding for infectious waste management found poor among biomedical waste management staff (32%). Uddin et al.[20] found the similar result in a study at Faridpur hospital.
Sanjeev et al.[21] about 40% of the respondents were aware of amalgam separators. Amalgam separators are devices designed to remove amalgam waste particles completely in dental office discharge. These separators remove the particles using different techniques such as sedimentation, filtration, centrifugation, or ion exchange which was similar to a present study (38.6%).
There are no reliable data available of the quantum of waste generated per person per day either in indoors or outdoor patient in Indian Hospital, particularly in Vellore. Even there is no uniformity in the data on the quantum of biomedical waste being generated.
The variation in the quantum of waste generation differs not only from country to country but also within the country which depends on the type of health-care establishment, hospital specialization, proportion of reusable items employed in the health-care center’s and proportion of patients treated on a day-care basis.[22]
From the data available from Singh et al.[22] where the average daily waste generated from anatomical waste is 5.6 kg.
In the present study, the average daily waste particularly the anatomical waste shows high quantity, i.e. 2 kg/day.
Sudhakar et al.[23] conducted among private dental practitioners in Bangalore city, India, wherein 39.1% of the respondents were not segregating excess mercury/or amalgam but were discarding it to regular Garbage. This result is similar to a present study (58%).
As far X-ray fixer is concerned, we know the fact that X-ray fixer is considered a hazardous waste because of its high silver content. Developer solutions should not be mixed with fixer solutions. The resulting solution is hazardous. The fixer can be recycled and the developer can be sewered.
In a study by Mushtaq et al.,[24] waste X-ray developer and waste X-ray fixer were not collected in separate bottles, rather they are wasted through main wastewater sewage system, therefore posing health threats it needs revolutionary changes in the ultimate fate of X-ray fixer which was in accordance to the present study (16%).
All the surveyed setups were found discharging their dangerous waste directly down the drainage waste and also thrown in the garbage.[25-27] These results are in comparison to other studies conducted were similar to the present study.
The BMW management practices in the hospital were satisfactory, except for a deficiency in use of needle-cutters in clinics (63.3%) which were similar to the study by Mathew et al.[28] and Benjamin et al. (41%).
The practice of reporting injuries resulting from improperly disposed of biomedical waste was found to be completely absent among the staff. Stein et al.[29] in their study reported that among doctors and nurses, only 37% reported that they ever suffered needle stick injury 39.3% in the present study.
Maroof et al.[30] reported that 43.3% of the study subjects had heard of hepatitis B. The BWM in the hospital is more in contact with the patients and therefore at greater risk of acquiring hepatitis B and their knowledge is very deficient which was similar to the present study.
However, in the present study, the majority of respondents (22.6%) had not received any formal training in biomedical waste management. Similar result was noted by Akter et al.[31] and Madhukumare et al.[32] while performed similar type of research among tertiary healthcare workers.
The present cross-sectional study was carried out to assess the knowledge and practices of healthcare professionals about biomedical waste management in dental clinics. This study showed that of 150 health-care professional’s doctors (82%) had better knowledge compared to other health-care professionals regarding disposal of biomedical waste, this finding was corroborated by the study done Holla et al.[33] (84%).
RECOMMENDATIONS
-
Adequate supplies and equipment should be available in all departments to take care of wastes.
-
Collected information on various methods of disposal and updated technology should be made available to all categories of health-care personnel.
-
Compulsory training for their health-care personnel from accredited training centers.
-
Easy color coding for BMW disposal bags should be developed in local languages for the betterment of sanitary workers and general public awareness.
-
Hospital superintendents, Government Health administration, and public awareness need to pay their specific attention to this important issue of health and hygiene.
-
Intensive training or workshops program at the regular time interval for all staff working in hospitals and clinics, and a system of monitoring and surveillance about the practice of day to day BMW management should be evolved.
-
Proper BMW disposal practices could be accentuated in health-care personnel if they are put under direct supervision and direct surveillance.
-
Reasonable amount of fund must be provided for waste management.
-
There is dire need of segregation of waste at source besides following color code system of waste management.
-
To install proper incinerators in all the cities.
-
Universal precautions should be adapted while dealing with hazardous and infectious waste.
-
Yielding posters with and leaflets should be used to for providing such education.
-
Endorsing the principles of green dentistry which reduces waste and pollution, saves water, energy, and money is high-tech and supports a wellness lifestyle.
CONCLUSION
Occupational safety is a prime concern. Being a recent field of interest, the level of knowledge on this concept is insufficient and needs to be increased to raise awareness to the environmental aspects.
Protected and effective execution of waste management rules is not only a legal necessity but also a social liability.
Lack of knowledge, motivation and cost factor are some of the hurdles faced in proper waste management.
The importance of training regarding biomedical waste management cannot be overemphasized.
Health-care professionals and government should work together to develop standard feasible policies for BMW management.
The study revealed a lack of knowledge in different tiers of health-care providers which adversely affects their practice.
CONCLUSIONS
The present study is done on a small scale. The results of this study reinforce the belief that the internet is becoming a valuable asset to the dental profession.
Tomorrow’s Internet, however, may be very different from the Internet of today. The Internet’s driven by a massive ongoing conversion to electronic commerce, which will drive high-speed access and more convenient connections. Dentistry can only benefit.